
How To Get a Pharmacovigilance Certification in West Virginia: Everything You Need to Know in 2025–2026
West Virginia looks small on the trial map—but PV hiring doesn’t care about size; it cares about speed, accuracy, and audit-readiness. Health systems in Charleston, Morgantown, Huntington, Parkersburg, Wheeling and regional CROs need certified contributors who can hold SUSAR clocks, code MedDRA cleanly, and write crisp narratives. This guide gives you a WV-specific execution plan: which accredited certification to choose, which proof artifacts to assemble, and how to secure remote/hybrid drug-safety roles across the Mid-Atlantic. For phrasing and documentation style, mirror CCRPS’s state playbooks such as New York, North Carolina, Ohio, and Pennsylvania.

1)West Virginia’s PV Reality in 2025–2026: Why Proof Beats Pedigree Here
WV employers value repeatable PV process over brand names. If you can control Day-7/15 clocks, code MedDRA consistently, and author inspection-ready narratives, you’ll unlock hybrid/remote roles that cover WV plus PA/OH/VA/MD. Calibrate your resume to inspection-aware phrasing modeled in CCRPS state playbooks like Pennsylvania, New York, and North Carolina; mirror their clock-start language, expectedness logic, and QC sign-off patterns. For documentation cadence, borrow the checklist discipline from Oregon and Utah, then localize it to WV hospital research workflows.
Address pain points in interviews with mini-SOPs: a timeline-control SOP, a coding synonym list (LLT→PT→HLT→SOC), a QC rubric with pass thresholds, and a CAPA template for late SUSARs—an approach echoed in Rhode Island and Washington. Lean teams in Charleston–Morgantown–Huntington reward operators who show measurable gains—think on-time SUSAR ≥98%, coding rework ↓30%, follow-up closure ≤5 days (phrase metrics like Pennsylvania and New York). Bring device-vigilance examples and combo-product nuances—WV systems notice that extra rigor (documentation tone similar to Oregon and Utah). Close interviews by mapping your artifacts to Mid-Atlantic coverage (WV+PA/OH/VA/MD) and cite CCRPS’s own West Virginia guide to signal regional literacy.
| Key Factor | 2025 Data (West Virginia) |
|---|---|
| Typical Entry Titles | Drug Safety Associate, PV Associate, Case Processor |
| Mid-Level Titles | Safety Scientist, Signal Scientist, PV Operations Lead |
| Senior/Lead Path | PV Manager, Aggregate Reports Lead, Benefit-Risk Lead |
| Remote/Hybrid Share | ≈60% roles hybrid/remote (Mid-Atlantic coverage) |
| Entry Salary | $68k–$82k base + benefits (hybrid stipends vary) |
| Mid Salary | $85k–$104k; signal/aggregate experience trends higher |
| Senior Salary | $108k–$135k+; leadership & inspection history lift bands |
| Hiring Hubs | Charleston, Morgantown, Huntington, Parkersburg, Wheeling |
| Core Safety Systems | Argus, ArisGlobal LifeSphere, Veeva Safety, Vault QMS |
| Coding Standards | MedDRA v26+; WHO-Drug/WHO-DD product dictionary |
| Case Sources | Clinical trials, post-market, literature, PSPs, spontaneous reports |
| Regulatory Outputs | SUSARs, expedited ICSRs, PBRER/PSUR, DSUR, RMP |
| US/EU Timelines | Serious/SUSAR 7–15 days; others per label and region |
| Signal Process | Detection → Triage → Validation → Analysis → Recommendation → Tracking |
| Audit Hotspots | Clock-starts, expectedness, seriousness, narrative quality, coding QC, CAPA proof |
| Device Vigilance | WV health systems use device PV; combo product nuance helps |
| Interview Proof | 2 narratives + coding rules + E2B(R3) exports + PBRER shell |
| First 90-Day Wins | SUSAR calendar, follow-up SOP, synonym list, QC rubric, CAPA library |
| Cross-Over Talent | RN/PharmD/CRA/Med Writer/Epidemiology → rapid PV ramp |
| Time to Offer | 8–14 weeks with portfolio + mentor references |
| Networking Targets | Hospital research offices, CROs, academic safety teams |
| WV Edge | Lean teams, multi-state coverage, faster promotion cycles |
| Common Gaps | Vague narratives, weak expectedness logic, missed follow-ups |
| Skills Most Screened | Narratives, MedDRA hierarchy, E2B(R3), CAPA writing, signal notes |
| Literature Screening | Cadence, de-duplication, abstract narrative sourcing |
| Aggregate Rhythm | Lock shells early; rolling tables; QC initials tracked |
| Regulators to Know | FDA/FAERS, EMA/EudraVigilance, MHRA/Yellow Card, Health Canada |
| Long-Term Path | PV Manager → Signal Lead → Benefit-Risk → Global Safety leadership |
2) Step-by-Step: Earning a WV-Ready Pharmacovigilance Certification (No Wasted Motion)
1) Pick an accredited, skills-first PV certificate.
Prioritize case labs, MedDRA v26+ practice, E2B(R3) exports, SUSAR clock controls, and aggregate report shells. Align wording with competitive markets like New Jersey and Midwest hubs like Ohio.
2) Build a portfolio while training.
Deliver two anonymized narratives, a coding rulebook (LLT→PT→HLT→SOC), a SUSAR calendar, and a PBRER skeleton. Model your document tone after Pennsylvania and Oregon.
3) Log practice hours with evidence.
If you’re new, simulate end-to-end cases: intake → seriousness/expectedness → narrative → MedDRA → QC → E2B(R3) → submission proof. Adopt the checklist mindset highlighted in Tennessee and WV’s own inspection tone seen in West Virginia CRA.
4) Rehearse regulator scenarios.
Flashcards for US/EU/UK/Canada timelines, listedness vs expectedness, seriousness, follow-ups, and CAPA drafting. Verify your clock-start triggers. Keep submission logs as proof—an approach favored by Rhode Island and Washington.
5) Secure WV-savvy mentorship.
Find mentors with Mid-Atlantic coverage (WV+PA+OH+VA). Use regional literacy from Virginia and neighbors like North Carolina to calibrate expectations.
3) Skills West Virginia Screens For (and Exactly How to Prove Each One)
Case intake → closure with proof.
Show the full chain: intake note → seriousness/expectedness → MedDRA LLT→PT→HLT→SOC → narrative → QC checklist → E2B(R3) export → submission record. For inspection tone and bullet phrasing, study Pennsylvania and New York.
MedDRA mastery (rework killer).
Write a coding rulebook that resolves synonyms and ambiguous terms, including device vigilance wording. Model process clarity after Oregon and Utah.
Expedited reporting discipline.
Maintain a clock-start matrix (US/EU/UK/Canada), calendar reminders, and a CAPA template for misses. Keep submission evidence/logs—language echoed in Rhode Island and Washington.
Signal & benefit-risk.
Draft a 1-page signal memo: detection method → triage criteria → validation → analysis → recommendation → tracking. For analytical tone, mirror North Carolina and Ohio.
Aggregate reports.
Lock a PBRER shell early. Maintain rolling tables, tracked changes, and QC initials. Add device-combo nuances where relevant. Documentation discipline aligns with Virginia and Wisconsin.
Your #1 Blocker to PV in West Virginia?
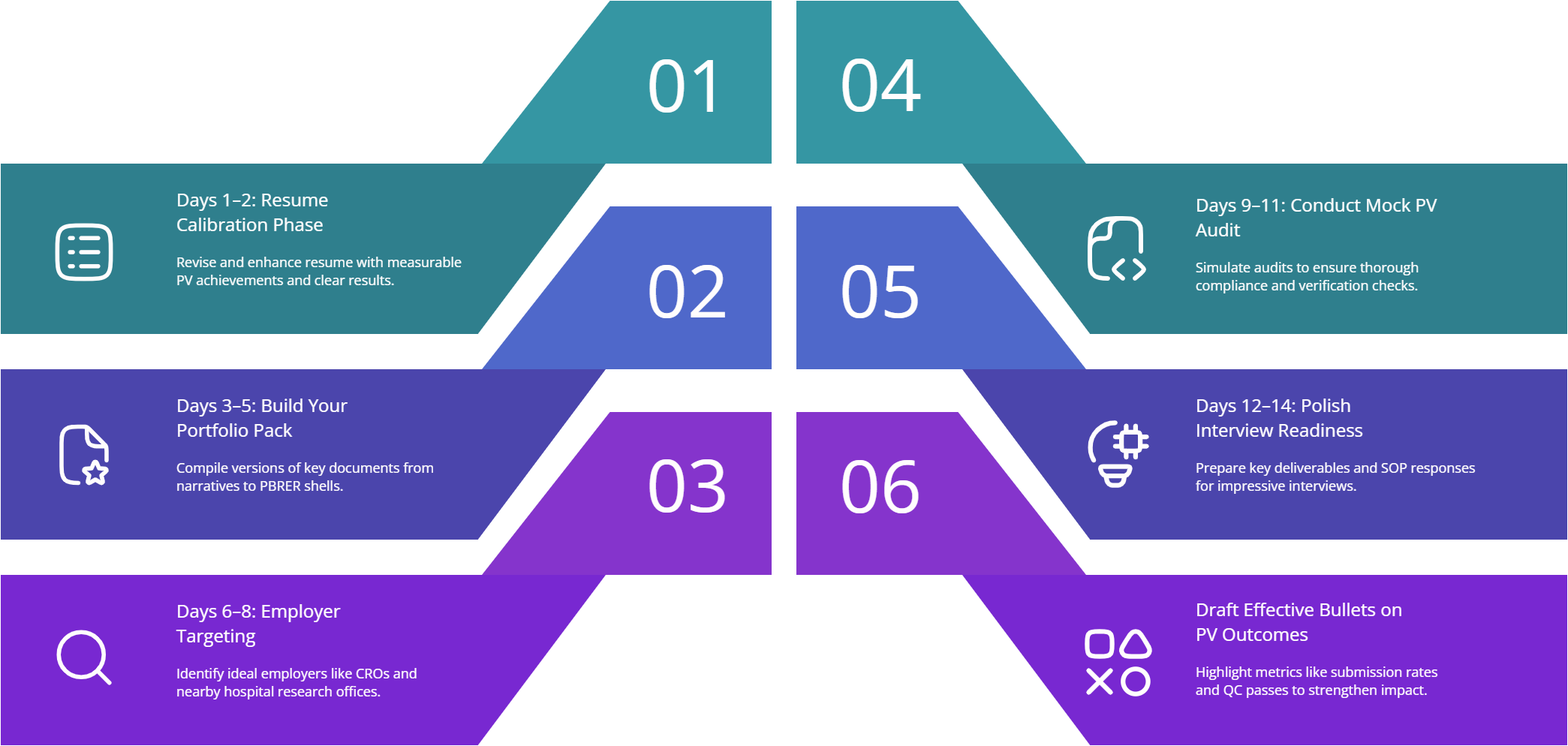
4) A 14-Day WV Execution Plan (From Learning to Offer)
Days 1–2 — Resume calibration.
Rewrite bullets around measurable PV outcomes (on-time SUSAR %, QC pass %, rework reduction, follow-up closure times). Borrow phrasing from New York and Pennsylvania.
Days 3–5 — Portfolio pack.
Bundle 2 anonymized narratives, coding rulebook, timeline grid, signal memo, PBRER shell. Keep a versioned index. Structuring cues: Oregon and Tennessee.
Days 6–8 — Employer targeting.
Shortlist hospital research offices, CRO satellites, and device safety teams. Pitch hybrid coverage (WV + PA/OH/VA/MD). Demonstrate regional literacy by citing West Virginia CRA, Ohio and Virginia.
Days 9–11 — Mock inspection.
Run a 10-point PV audit: clock-starts, expectedness, seriousness, narrative clarity, coding QC, submission proof, CAPA, retraining records, literature triage, version control. For rigor/style, review Rhode Island and Washington.
Days 12–14 — Interview sprints.
Answer with mini-SOPs: “Here’s my Day-15 calendar, coding rules, follow-up letter, E2B(R3) export, and CAPA.” Close with hybrid bands (e.g., 2–4 days/month onsite, rest remote). Reinforce with WV CRA plus neighbors Ohio and Virginia.
5) Career Ladders, Compensation, and How to Accelerate to Signal/Aggregate Leadership
Year 0–1 — PV Associate/Case Processor.
KPIs: on-time expedited submissions, MedDRA QC ≥98%, narrative clarity, follow-up closure time. Phrase results like high-bar markets New York and Pennsylvania.
Year 1–3 — Safety Scientist.
Own signals, aggregate inputs, deviation CAPAs, literature cadence. Use coding rulebook to cut rework. Benchmark phrasing via North Carolina and Ohio.
Year 3–5 — PV Manager/Aggregate Reports Lead.
Deliver PBRER/PSUR/DSUR on schedule; coach juniors on narratives/coding; institutionalize QC checklists and version control. Tone aligns with Virginia and Wisconsin.
Compensation levers.
Negotiate with metrics: on-time SUSAR %, coding rework delta, aggregate cycle time, audit findings closed, hybrid multi-state coverage (WV+PA/OH/VA/MD). Regional leverage language echoes Washington and Pennsylvania.
6) FAQs: Pharmacovigilance Certification in West Virginia (2025–2026)
-
Hands-on case labs, MedDRA practice, E2B(R3) exports, and aggregate report shells. Assemble a portfolio (2 narratives, coding rules, SUSAR calendar, PBRER shell). Match phrasing to Pennsylvania and North Carolina.
-
Bring a clock-start matrix, alarms, and submission logs. Add a CAPA template and retraining notes. This timeline discipline mirrors Rhode Island and Washington.
-
-
-
Yes—especially in health-system device safety and combination products. Show device-specific coding examples and link to risk-file logic. Documentation habits can echo Oregon.
-
Typically $68k–$82k base in WV; negotiate higher with on-time SUSAR rates, coding QC ≥98%, and aggregate cycle-time wins. Use regional framing from Ohio and inspection-awarePennsylvania.
-