
Essential Training Requirements for Research Assistants
Research assistants sit close to the work that makes or breaks a clinical trial: source notes, participant contact, lab coordination, specimen handling, document control, data entry, and safety follow-up. That means training cannot be vague, rushed, or treated like onboarding paperwork. A research assistant who understands GCP compliance, research ethics, study documentation, and laboratory best practices becomes a protection layer for participants, data quality, and inspection readiness.
1. Training Requirements for Research Assistants Begin With Role-Specific GCP Competence
A research assistant needs training that matches the tasks they actually perform, the trial risks they touch, and the decisions they must escalate. ICH E6(R3) describes GCP as the international ethical and scientific quality standard for designing, conducting, recording, and reporting trials involving human participants, with emphasis on participant rights, safety, well-being, and reliable results. For research assistants, this connects directly to GCP compliance essentials, clinical research coordinator responsibilities, clinical trial documentation techniques, and clinical trial data integrity.
The first pain point is over-general training. Many sites give research assistants one GCP certificate, one protocol slide deck, a delegation log signature, and a quick EDC login. Then the assistant is expected to handle source prep, participant reminders, lab kits, document uploads, screening support, query follow-up, and visit tracking without enough scenario practice. That creates quiet risk. A missed visit-window calculation can become a protocol deviation. A poorly labeled specimen can damage laboratory quality. A vague phone note can weaken adverse event reporting. A late upload can create gaps in regulatory document management.
Research assistant training should be built around a task map. The site should list every task the assistant performs, the training needed for that task, the supervising role, the source of truth, the escalation trigger, and the documentation evidence. FDA guidance on investigator responsibilities states that when investigators delegate tasks, they remain responsible for adequate supervision of delegated staff, and the guidance focuses on protecting human subjects while maintaining data integrity. That is why PI oversight, essential GCP training requirements, clinical trial audits, and inspection readiness all depend on training that is traceable, role-specific, and current.
2. Research Assistants Must Be Trained on Ethics, Consent Boundaries, and Participant Protection
Research assistants often become the first person a participant contacts when something changes. That makes ethics training more than a background requirement. The Belmont Report explains informed consent through information, comprehension, and voluntariness, and it identifies respect for persons, beneficence, and justice as core human research principles. A research assistant who understands these principles will know when a participant’s confusion, pressure, fear, language barrier, or medical concern needs escalation to the coordinator, investigator, or consent-delegated staff. This strengthens informed consent procedures, ethical conduct in clinical trials, patient safety oversight, and regulatory responsibilities for PIs.
Consent-boundary training is critical because many research assistants support consent logistics without being authorized to conduct consent. They may print the correct version, confirm dates, prepare private space, schedule interpreters, witness signatures where allowed, or document that the participant received a copy. They should also know where their role stops. Explaining risks, comparing treatment alternatives, reassuring a participant about safety, or encouraging enrollment should be handled by properly delegated staff. This is especially important in trials with randomization, blinding, placebo-controlled designs, and primary or secondary endpoints that participants may misunderstand.
Participant-protection training also includes privacy, respectful communication, vulnerability awareness, and fair access. A research assistant should know how to protect identifiers, avoid discussing participants in public spaces, use approved contact methods, document participant complaints, and escalate medical questions. A small mistake can feel harmless in the moment: sending a reminder to the wrong number, leaving detailed voicemail content, copying the wrong attachment, or discussing schedule details near a waiting-room desk. These mistakes can damage trust and create compliance exposure. Strong habits connect research compliance and ethics, clinical trial patient education resources, effective patient retention strategies, and clinical trial volunteer registries.
3. Documentation, Data Entry, and Source Quality Training Protect the Trial From Silent Failure
Source documentation training is one of the biggest requirements for research assistants because many RA tasks create the raw evidence later used by coordinators, CRAs, sponsors, auditors, and inspectors. A research assistant may record participant contact attempts, prepare visit source packets, scan lab reports, upload documents, transcribe visit dates, track specimen shipments, enter low-risk data fields, or respond to administrative queries under supervision. Each action needs accuracy, attribution, timing, and traceability. This directly supports managing study documentation, case report form best practices, clinical trial data review, and clinical trial data integrity for PIs.
The pain point is that documentation errors often look small until they create a credibility problem. “Called participant, no answer” may be acceptable for scheduling, but it is weak if the call was part of safety follow-up. A scanned lab report without date, source, or review status can create confusion during monitoring. A corrected visit date without reason can trigger audit-trail questions. A lab kit shipment note without tracking confirmation can become a specimen-chain problem. RAs need examples of good source notes, poor source notes, acceptable corrections, late entry language, and source-to-EDC reconciliation. This aligns with remote and on-site monitoring visits, site monitoring visit preparation, risk-based monitoring, and handling clinical trial audits.
Data-entry training should include system access rules, source alignment, query etiquette, audit trail awareness, and escalation triggers. A research assistant should never “fix” data to make pages look clean. They should understand that EDC entries must reflect source, source gaps must be escalated, and query responses should address the documented issue without inventing facts. If the source is wrong, the source needs correction. If the EDC is wrong, the EDC needs correction. If both are unclear, the issue needs review. This is where clinical trial technology innovations, directory of clinical trial templates, interactive checklist generators, and GCP self-assessment tools become practical training aids.
Where is your research assistant training gap most likely to hurt the study?
Choose one risk. The answer shows which competency needs immediate reinforcement before the next monitoring visit.
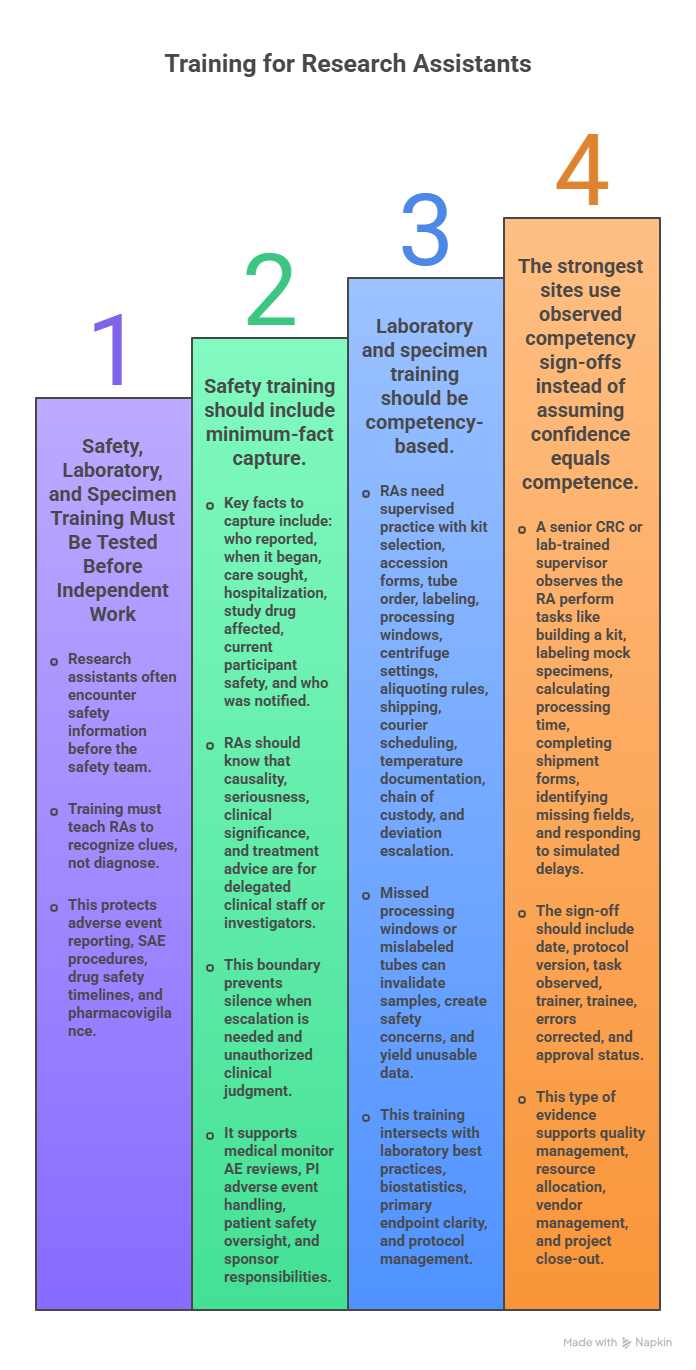
4. Safety, Laboratory, and Specimen Training Must Be Tested Before Independent Work
Research assistants often touch safety information before the safety team sees it. They may answer calls, schedule urgent visits, review messages, collect symptom updates, prepare AE follow-up packets, scan outside records, or notice medication changes. Their training must teach them to recognize clues rather than diagnose. “I went to the ER,” “my doctor stopped one medicine,” “I had chest tightness,” “I was admitted overnight,” “my lab was abnormal,” or “I missed study medication because I felt sick” should trigger escalation. This protects adverse event reporting, SAE reporting procedures, drug safety timelines, and pharmacovigilance safety monitoring.
Safety training should include minimum-fact capture. The RA should know how to record who reported the issue, when it began, whether care was sought, whether hospitalization occurred, whether study drug was affected, whether the participant is safe now, and who was notified. They should also know that causality, seriousness classification, clinical significance, and treatment advice belong to delegated clinical staff or investigators. This boundary prevents two opposite errors: silence when escalation is needed and unauthorized clinical judgment when the RA wants to help. It supports medical monitor AE reviews, PI adverse event handling, patient safety oversight, and clinical trial sponsor responsibilities.
Laboratory and specimen training should be competency-based. Reading a lab manual once cannot prove readiness. RAs need supervised practice with kit selection, accession forms, tube order, labeling, processing windows, centrifuge settings where applicable, aliquoting rules, frozen or ambient shipping, courier scheduling, temperature documentation, chain of custody, and deviation escalation. One missed processing window can invalidate a sample. One mislabeled tube can create participant safety concerns and unusable endpoint data. This is where laboratory best practices, biostatistics in clinical trials, primary endpoint clarity, and clinical trial protocol management intersect.
The strongest sites use observed competency sign-offs instead of assuming confidence equals competence. A senior CRC or lab-trained supervisor watches the RA build a kit, label mock specimens, calculate processing time, complete a shipment form, identify missing fields, and respond to a simulated courier delay. The sign-off should show date, protocol version, task observed, trainer, trainee, errors corrected, and approval status. This type of evidence supports quality management strategies, clinical trial resource allocation, vendor management, and project close-out procedures.
5. Training Records Must Prove Readiness, Supervision, and Continuing Competence
A training record should prove more than attendance. It should show that the research assistant was qualified before performing assigned tasks, trained on the correct protocol version, delegated appropriately, supervised adequately, retrained after changes, and evaluated when performance issues appeared. ICH E6(R3) and FDA’s E6(R3) materials emphasize proportionate quality, critical thinking, clarified responsibilities, and modern trial conduct expectations. For RAs, that means training files should connect GCP training requirements, delegation and PI oversight, audit preparation, and CRA inspection readiness.
The common inspection weakness is mismatch. The RA is delegated to collect vitals, but the vitals training is missing. The RA uploads safety letters, but eReg training came later. The RA enters data, but EDC access began before system training. The RA supports a visit after an amendment, but amendment training was completed after the visit date. These mismatches tell an inspector that the site may have assigned work before proving readiness. A clean record connects CV or résumé, role description, GCP certificate, protocol training, task-specific competency, system access dates, delegation start dates, amendment training, retraining records, and supervision notes. This also strengthens regulatory document management, site monitoring visit workflows, clinical trial documentation, and interactive GCP compliance self-assessment.
Continuing competence matters because trial conduct changes. Amendments alter procedures. Safety letters change risk awareness. New lab manuals change processing steps. EDC updates change query workflows. CAPA findings reveal weak habits. Staff turnover changes supervision patterns. A research assistant trained once at start-up may become risky three months later if the trial has changed and retraining has not followed. Sites should retrain after protocol amendments, consent updates, new tasks, recurring errors, monitoring findings, lab manual changes, safety updates, privacy incidents, system updates, and delegation changes. That approach supports clinical trial amendments, handling protocol deviations, leadership and team management, and clinical research continuing education.
Supervision should be visible in the record. A PI or senior study lead should be able to explain how the RA was trained, which tasks they perform, who reviews their work, how errors are corrected, and when independence was approved. A strong training system includes onboarding checklists, task competencies, shadowing logs, observed performance forms, escalation drills, periodic quality checks, and targeted retraining. The result is a site where RAs handle routine tasks confidently and escalate risky issues quickly. This helps clinical trial project managers, clinical research associates, clinical research coordinators, and principal investigators trust the workflow.
6. FAQs About Essential Training Requirements for Research Assistants
-
Every research assistant should complete GCP training, human subject protection training, protocol training, role-specific delegation training, source documentation training, privacy training, safety escalation training, lab or specimen handling training if applicable, system-access training, and site SOP training. The exact mix depends on assigned tasks, study risk, local policy, and sponsor requirements. A strong training file links each task to proof of readiness. This supports research assistant documentation skills, GCP training requirements, research compliance and ethics, and laboratory best practices.
-
Research assistants can support informed consent only within their delegation, training, local policy, and protocol requirements. They may help with scheduling, room setup, document preparation, version checks, interpreter coordination, or administrative support. Explaining risks, answering medical questions, assessing understanding, and obtaining consent should be performed by properly delegated and qualified staff. The site should define these boundaries before the first participant visit. This protects informed consent compliance, ethical conduct, PI regulatory responsibilities, and CRC responsibilities.
-
The most important documentation skills are accuracy, timeliness, attribution, source clarity, correction discipline, version control, and escalation documentation. RAs should know how to write clear contact notes, file documents correctly, maintain visit checklists, track missing records, avoid undocumented corrections, and align source with EDC entries. Weak notes create rework during monitoring and can make a compliant visit look unreliable. Strong training should include mock source notes and supervisor review. This connects to case report form best practices, clinical trial data review, site monitoring preparation, and clinical trial documentation.
-
Research assistants should be trained to recognize possible AE and SAE clues, capture minimum facts, document participant contact accurately, and escalate quickly to the correct clinical or study lead. They should avoid making medical judgments unless delegated and qualified. Training should include scenarios involving hospitalization, new symptoms, medication changes, abnormal labs, emergency visits, missed doses, and participant complaints. This strengthens AE reporting techniques, SAE reporting procedures, drug safety timelines, and clinical trial safety monitoring.
-
Research assistant training should be updated whenever the protocol, consent form, lab manual, safety information, system workflow, delegation, SOP, or assigned task changes. It should also be refreshed after monitoring findings, CAPA actions, repeated errors, privacy issues, staff role changes, or new responsibilities. Annual training can help, but task-based retraining is more protective because it follows real trial risk. This supports clinical trial amendments, protocol deviation management, quality management strategies, and continuing education resources.
-
An inspection-ready training record shows the RA’s role, qualifications, GCP training, protocol training, task-specific competency, system access training, delegation dates, amendment training, retraining evidence, and supervision history. The dates should make sense: training should come before delegation, system access should follow training, and amendment training should occur before amended procedures are performed. The record should prove competence, not attendance alone. This protects clinical trial audit readiness, CRA inspection readiness, regulatory document management, and GCP self-assessment.